MSC (MicroSave Consulting) conducted a workshop titled “Digital Transformation of Postal Operators: Massive outreach, opportunities and challenges” on the 24th of February, 2021.
This webinar was designed to promote thinking and action on the digital transformation of postal operators in order to leverage their outreach to deliver real financial inclusion. It focused on three aspects:
The opportunities and competitive advantages enjoyed by postal operators;
The challenges postal operators have faced or are likely to face as they digitize; and
The various business models for postal operators.
00:-2:11 Doreen Njau, Communications Manager—Anglophone Africa, MSC kicks off the session, welcomes partipants, and gives details of the flow of events.
10:28–11:43 Juliet Ongwae, DFS Specialist at MSC introduces the first topic: Postal operators, the pandemic, and finding a new purpose.
11:43–13:46 Victoria Griffith, Program Officer, Financial Services for the Poor, the Bill & Melinda Gates Foundation talks to respond to question 1. The pandemic has provided a great opportunity for digital financial services and e-commerce activities by postal operators. What strategies can shape the future of postal digital transformation?
14:34–21:19 Raphael Lekolool, CEO, Kenya Post Office Savings Bank answers question 2. What is the impact of the pandemic on your services and what strategies have you put in place to handle the changing demand?
21:46–27:47 Jayanthy Venkatramu, CEO, India Post Payment Bank answers question 3. What are some of the opportunities that the pandemic offer to the postal sector?
28:25–36:15 Siva Somasundram, Director, Directorate of Policy, Regulations, and Markets (DPRM), Universal Postal Union responds to question 4. The pandemic has spotlighted the crucial need for international collaboration in all domains. How has UPU supported the postal operators in offering inclusive social, logistics and financial services?
36:35–40:39 The panelists respond to round one of questions from the audience.
Question 1) Most of the postal companies operating in rural Africa are government-owned. Digital transformation of these companies for financial inclusion agenda will need effective PPP. Can you share any knowledge guide on this?
Question 2) Speakers have talked about payments, transfers, … are some of your institutions developing a credit offer for your customers? (be it digital credit or more traditional credit)
40:39–41:14 Juliet Ongwae, DFS Specialist at MSC introduces the second topic:Digital postal services – Strategic insights and way forward for postal digitization
41:12–48:14 Raphael Lekolool, CEO, Kenya Post Office Savings Bank answers question 1: What are some of the challenges you have faced in the digital transformation journey and what culture change is needed to facilitate this?
49:02 -52:50 Jayanthy Venkatramu, CEO, India Post Payment Bank answers question 2: As you provide last mile financial services across India, what are the key lessons learnt to overcome challenges such as identifying and managing effective partnerships, digital identity and authentication, low literacy levels, interoperability, customer trust in digital financial services?
53:26– 55:44 Victoria Griffith, Program Officer, Financial Services for the Poor, the Bill & Melinda Gates Foundation talks to respond to question 3: How can the postal operators leverage on the dynamic growth in data analytics, artificial intelligence, IoT, cloud computing, open APIs, etc.?
56:04–1:03:40 Siva Somasundram, Director, Directorate of Policy, Regulations and Markets (DPRM), Universal Postal Union responds to Question 4: What is UPU’s strategic direction that will enable it to support the development of a digital postal ecosystem (standardization, digitalization, e-commerce, transport, e-cash)?
1:04:31– 1:08:59 Jayanthy Venkatramu, CEO, India Post Payment Bank answers question 5: Do you have any partnerships with fintechs and what are the options and possibilities for Posts to leverage fintechs to accelerate and simplify their digital transformation and how can you effectively collaborate given the difference in your business models, culture, technology?
1:09:23–1:10:09 Victoria Griffith, Program Officer, Financial Services for the Poor, Bill and Melinda Gates Foundation talks responds to Question 6: Is there a role for a specialized accelerator that can identify Post’s specific needs and accelerate fintechs solutions to address them?
1:10:21– 1:21:33 The panelists respond to round two of questions from the audience
Question 1: Are there security issues faced by Postal personnel while offering financial services in rural areas across globe?
Question 2: What are the common collaterals used in rural areas and what is the effectiveness of the collaterals in motivating repayment of credit?
Question 3: Rural youths (who are digital savvy) are moving to urban centers for greener pastures, leaving the aged folks behind. How will digital postal systems for financial inclusion benefit the rural aged who are known not to be digital friendly?
1:21:52–1:29:09 Juliet Ongwae, DFS Specialist at MSC opens the floor to the panelists for their parting shots.
1:29:20–1:29:52 Juliet Ongwae, DFS Specialist at MSC speaks of the key highlights from the workshop.
1:30:32–1:31:45 Graham Wright, Group Managing Director, MSC, presents the concluding remarks.
COVID-19 has changed the way consumers use payment instruments fundamentally. The might of digital payments came to the fore as it helped protect vulnerable segments through seamless and quick government-to-person (G2P) payments. Digital payments offered convenient and contactless modes of payment as well as collection to customers and businesses respectively. This report analyzes the trends of various payment system indicators through 2020 and identifies the forces behind such trends. It also explores the lives of three Indian women from different socio-economic backgrounds as they go about their financial lives and how they navigated various barriers and opportunities during the pandemic.
Part I of this focus note discussed how free power to the agriculture sector has led to the overexploitation of groundwater in India and the response of the Punjab government—a pilot program for Direct Benefit Transfer in Electricity (DBTE). This part highlights major challenges from the demand and supply-side perspectives. It also recommends ways to address these challenges and explores how DBTE can be scaled up in other states as well.
Governments around the world are rushing to mitigate the economic fallout from the COVID-19 pandemic, particularly on lower and middle-income groups. Among the range of proposed responses, the idea of a Universal Basic Income (UBI) has gained prominence. The United States has already begun providing cash transfers of USD 1,200 to all taxpayers, adjusted depending on income levels, while Spain is considering a minimum income transfer to vulnerable households to provide subsistence assistance and catalyze economic activity. The political and academic circles in India to have seen similar calls for a UBI in the country as a financial safety net to tide over an uncertain labor market in a post-COVID-19 scenario. Given the renewed interest in UBI, this blog will analyze the suitability of UBI in the Indian context.
1. What is UBI?
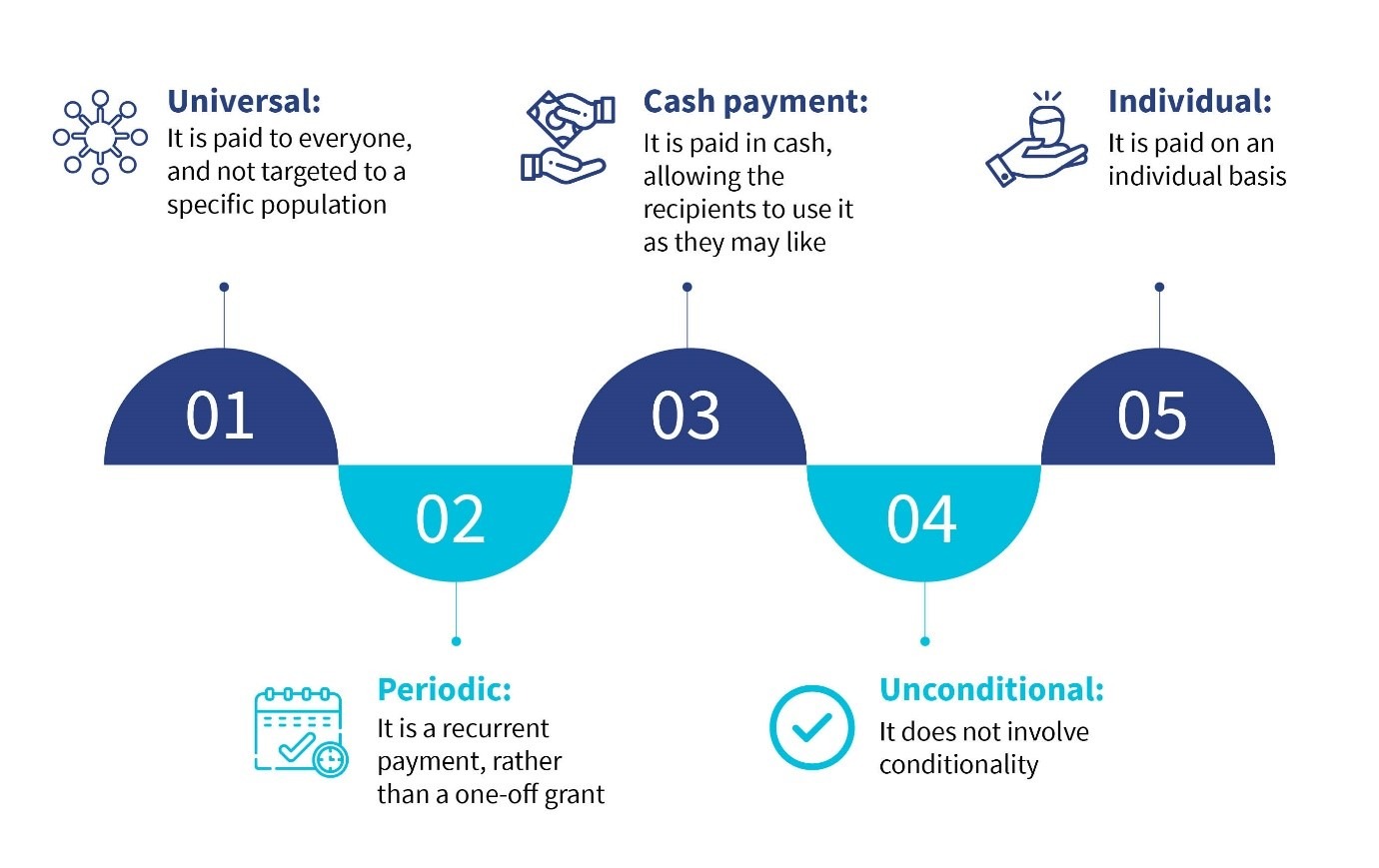
Universal Basic Income has taken distinct forms in different contexts depending on historical and geographical factors. While there might not be a standard definition of UBI, the fundamental tenants include:
The concept of a UBI has both proponents and detractors. In developed countries, proponents of UBI recognize it as a solution to rising inequality and unemployment precipitated by technological advancements. Many see it as an alternative to the cumbersome “welfare state” and as a tool to alleviate poverty and provide a social safety net by covering subsistence needs. It is also favored in certain geographies like India because it gives more choice to recipients who currently receive in-kind transfers. Further, UBI seems appealing due to high administrative costs, leakages, barriers to enrolment, and inaccurate targeting that plague existing welfare initiatives.
On the other hand, critics of UBI, in both developed and developing countries, argue that a UBI would not be fiscally feasible to implement. They believe UBI defeats the objective of economic redistribution, discourages productive activity, and sparks inflation.
While a national implementation of UBI has not yet occurred, there have been multiple attempts to pilot variants of UBI or unconditional cash transfers at smaller scales in different countries. The charity GiveDirectly conducted trials on the effect of providing unconditional cash transfers to households in Siaya County in Western Kenya during 2014-2016. This exercise provides insights into the effects of a potential UBI.
The study found that 18 months after receiving the cash transfers, recipient households reported higher spending and an increase in durable assets. The higher demand for products and services also resulted in increased income among non-recipient households, which led to increased spending. However, the study reported that the gains accrued due to the income transfer were also unequal, with the households that were already well off gaining more than the poor households. This amplified the existing income inequalities in the village.
In Namibia, a two-year pilot project (2008-10) on a Basic Income Grant (BIG) was implemented in the Otjivero-Omitara area. All residents under the age of 60 received NAD 100 (USD 6.7) each month without conditions attached. The positive impact of the project included lower household poverty levels alongside increased attendance and lower dropout rates in schools. However, since the BIG was only implemented in Otjivero-Omitara, there was a significant migration towards the area, resulting in a 24% decrease in per capita income.
2. UBI in the Indian context
There have been trials on UBI in India, as well. SEWA Bharat, supported by UNICEF India, conducted a pilot on basic income transfer in the rural areas of Madhya Pradesh from 2012 to 2013. For the pilot, two categories of villages were identified—village and tribal village. For each category, a set of control villages was identified. An amount of INR 300 (USD 4) per adult and INR 150 (USD 2) per child as basic income was distributed unconditionally to all individuals within the village for 12 to 17 months, without imposing eligibility requirements. The results were encouraging with pilot villages performing better on parameters including open defecation, electricity connections, drinking water, nutrition, and food sufficiency when compared to the control group.
The Government of India’s (GoI) Economic Survey 2016-17 catalyzed discussions around UBI in India. These discussions explored the possible effect of UBI on various social development parameters, such as poverty reduction, social justice, and administrative efficiency. The discussion, in part, focused on the significant number of central sector and centrally sponsored sub-schemes (950) in India, such as food and fertilizer subsidies, employment guarantee programs, and scholarships, among other social assistance programs.
These schemes have varied targeting mechanisms, conditionality requirements, and modes of implementation. These targeting mechanisms are often crippled by exclusion and inclusion errors and high bureaucratic costs, resulting in inefficiencies and sub-optimal effectiveness. GoI’s Economic Survey 2016-17 posited that the implementation of UBI could substantially overcome these issues.
We could argue that over several decades, the GoI has taken small steps toward a quasi-UBI by implementing different modes of Direct Benefit Transfer (DBT) programs. The cash transfer in food subsidy pilot (2015) in the three union territories of Chandigarh, Puducherry, and Dadra and Nagar Haveli is an example of the shift from in-kind to cash transfers by the GoI. Under this pilot, all beneficiaries of the Public Distribution System (PDS) were entitled to receive cash transfers instead of rations received through PDS shops. Overall, beneficiaries were indifferent, yet the monetary savings realized by the GoI was significant in the range of 10% to 15% of the food subsidy bill.
Another unconditional and recurring income transfer program launched by the GoI in 2018 is PM Kisan, which entitles all landholding farmers to INR 6,000 (USD 80) annually. PM Kisan most closely mimics a UBI in India with the only conditionality being that the recipient must qualify as a landholding farmer, subject to a few exclusions. Over time, the program is expected to cover 140 million beneficiaries. These policy measures have created an environment in which the GoI could shift to UBI without significant friction in the future.
3. Designing an Indian UBI
The transition from existing government social welfare subsidy payments to UBI would require the GoI to address questions around eligibility, frequency, and amount of basic income to be provided. Yet questions remain around whether the government can comprehensively implement UBI, or if it would require a tailor-made approach. The following section details ways to address some of these foundational issues.
Is universality an option?
One of the core precepts of UBI is that it is universal in nature, which means all the citizens are, by default, beneficiaries. Adopting a universal approach in India would certainly result in higher government expenditures, while simultaneously ensuring that no citizens are excluded. This approach does away with the traditional mechanisms of delivering subsidies prevalent in India, which include defining a universe of beneficiaries and selecting from that universe.
Yet implementing UBI would be unaffordable in a country like India, where 22% of the population is classified as below the poverty line. This is because adopting a UBI would come at the cost of providing benefits to upwards of 78% of the population who would not need it immediately.
A better model for India would be to start with a targeted approach. Although this appears to be more affordable, it has its own set of challenges, including those around identifying the target segment (the poor) and limiting the flow of benefits to them. A targeted approach would require a robust database of beneficiaries and clear guidelines around exclusion parameters. Such an approach has always been subject to exclusion and inclusion errors. While wrongful inclusions lead to unnecessary expenditures, wrongful exclusions defeat the program’s purpose.
To address this, the GoI should develop a dynamic database in the long term, which can be used for beneficiary identification. The Socio-Economic Caste Census (SECC, 2011) can be utilized for immediate rollout since it captures the socio-economic profile of households in the country comprehensively. Although a targeted approach would stop short of a true UBI, it would have a significant impact on India’s population living below the poverty line. For a developing country like India, a quasi-universal basic income makes greater economic sense.
Can a UBI be a substitute for the existing welfare system?
The second major issue to be addressed is how a UBI would fit into the existing social welfare ecosystem in India. Estimates indicate that a UBI designed as a full supplement to existing social welfare schemes in India would add up to 13% of the current GDP and, therefore, is not fiscally feasible. On the other hand, the existing discourse (including the Economic Survey of 2016-17) rests on the idea that a UBI budget would replace all existing welfare programs. However, there are multiple issues with this approach.
First, rolling back programs meant to ensure food security and improve educational outcomes and sanitation, among others, would not only require backtracking on the achievement of human development goals but would not be politically viable. Welfare infrastructure, such as health care centers, plays an important role in nudging beneficiaries toward responsible behavior, particularly through social proofing.
Second, directly substituting UBI for the existing in-kind welfare programs ignores the additional transaction costs that would be borne by beneficiaries. These transaction costs include transport costs to access cash from banks, and wages lost as opportunity cost during travel and wait time. Third, some beneficiaries have expressed a preference for receiving in-kind subsidies—imposing a UBI ignores this preference. Fourth, clubbing existing benefits to make way for UBI will need a systemic overhaul because there are many backward and forward linkages. For example, PDS is linked to the Minimum Support Price (MSP) provided to farmers.
Finally, evaluation of cash transfer programs has thus far shown significant last-mile challenges including enrolment problems, Aadhaar seeding and authentication issues, delays in transfers, and gaps in grievance resolution.
Perhaps rather than view this as an “all or nothing” choice, policymakers should look at the middle road by implementing a supplementary income transfer to the targeted population. The GoI should retain existing in-kind programs that deliver necessities and enhance one’s quality of life, such as food security, sanitation, and education. Over time, once the GoI demonstrates that it has built a stable system that can reach the poorest through income transfers, it could revisit certain policies including giving beneficiaries the ability to select from different service providers, that is, existing public services or non-government providers.
This will empower beneficiaries by allowing them to decide how their social welfare funds could be spent. It could also potentially enhance the quality of public services by introducing competition with private or civil society organizations to attract business from the poor. In the long run, this could usher in greater accountability and efficiency among service providers.
Conclusion
Designing an Indian UBI requires an understanding of the constraints of the feasibility of universality and substituting existing welfare subsidies—and tailoring the program accordingly. In essence, a UBI in India could be implemented as a supplemental, unconditional, recurring cash transfer to the target population while keeping the existing welfare infrastructure intact. This approach mitigates concerns regarding financial viability by making incremental shifts to the welfare delivery ecosystem and introducing more choice to beneficiaries.
However, the GoI should first conduct a pilot study to understand the short-term and long-term effects that a basic Indian UBI would have on incomes, labor markets, communities, and beneficiary preferences. Only then should it throw its weight behind what is an extremely complicated and far-reaching program.
The Economic Survey of India reviews the developments in the Indian economy over the past financial year, summarizes the performance of major development programs, and highlights policy initiatives of the government and the prospects of the economy in the short to medium term.
Central Sector Schemes are the programs that are entirely and directly funded and executed by the central government.
Centrally Sponsored Schemes are programs that are implemented by state governments. However, the cost of these schemes is borne by the central and state government on a shared basis. Under the cost ratio, the larger portion is always borne by the central government.
The exclusion error fails to target the intended beneficiary population of the scheme. In contrast, the inclusion error causes funds to be spent on non-deserving populations, which leads to inefficiencies and budget increases.
Direct Benefit Transfer (DBT) is a mode of delivery of G2P payments launched by the GoI to transfer benefits and subsidies of various social welfare schemes directly into the bank accounts of beneficiaries.
Free or highly subsidized power to farmers in India has led to overconsumption of groundwater by the agricultural sector. The situation has reached a near-crisis level in many states due to these high subsidies. Unique models like Paani Bachao, Paise Kamao (Save water, earn money), the Direct Benefit Transfer in Electricity (DBTE) introduced in Punjab, offer a politically feasible and effective solution to the persistent issue of overuse of groundwater
Manage Consent
We use cookies to ensure your experience on MSC Global is secure, reliable, and optimized. By continuing to browse www.microsave.net, you agree to our use of cookies as described in our Cookie Policy.
Strictly Necessary Cookies
Always active
Required for website security, authentication, and essential functionality to provide a secure and optimized experience on Microsave.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Performance and Analytics Cookies
Used to improve website usability and reliability through anonymous analytics and usage insights on Microsave.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Functional Cookies
Remember your preferences such as language or region.